- Home
- Features Index
-
Features
Features
Breakthroughs in Undiagnosed Diseases: Identifying the Causes of Diseases and Uncovering New Illnesses through Genomic Analysis
2025/01/22
Have you ever heard of undiagnosed diseases? The term is used for cases where patients visit multiple hospitals and undergo numerous tests, yet the cause of their condition remains unknown. The past decade has seen the term become more common in Japan; today, more than 30,000 people across the country have been left without any recourse, with no clear diagnosis and their treatment options uncertain.
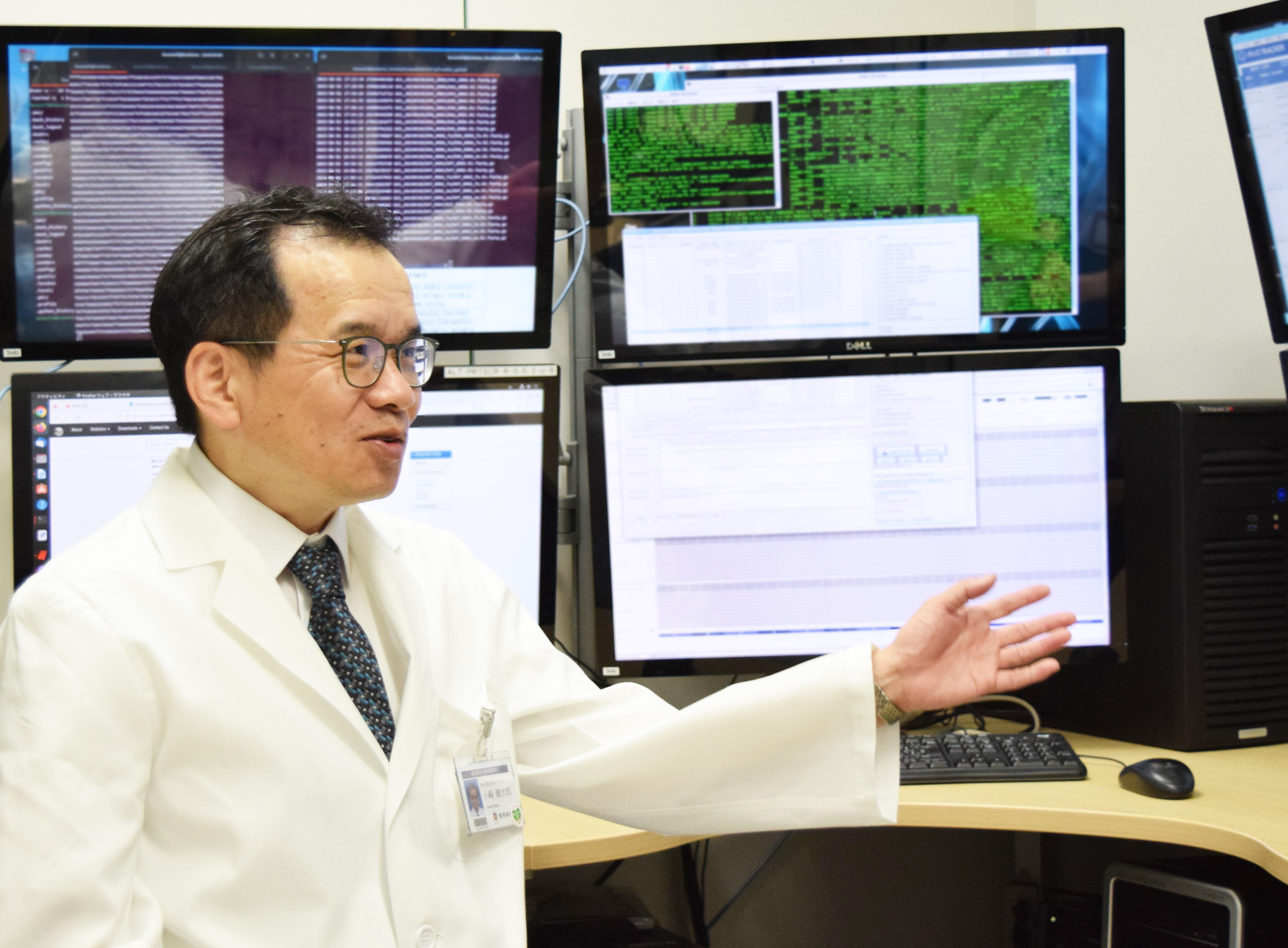
A team led by Prof. Kenjiro Kosaki, Director of the Center for Medical Genetics at the Keio University School of Medicine, has been working on a project to study the complete genome of these undiagnosed patients. Through the project, they have successfully diagnosed many cases and even discovered several new diseases ahead of other researchers around the world.
A Fascination with Molecular Biology and Developmental Biology Leads to a Career in Pediatrics
Despite his strong interest in basic medical sciences, such as molecular biology and developmental biology, Prof. Kosaki was driven by a desire to make a tangible impact as a clinician, which led him to study pediatrics, a field closely related to those disciplines. Students who study in a clinical department, including pediatrics, spend a period of time working at a regional hospital after graduation. Prof. Kosaki practiced at a large hospital in the northern Kanto region, providing pediatric care and emergency services, where he also took on many cases involving children with undiagnosed conditions.
After becoming a board-certified pediatrician, Prof. Kosaki pursued further studies at the University of California, San Diego, where he completed clinical training in diagnosing and treating patients with genetic disorders and earned certification as a clinical geneticist. During this time, he also engaged in genomic analysis research and earned his doctorate. Upon returning to Japan in 1998, Prof. Kosaki began leading a newly established clinical genetics division within the Department of Pediatrics, which specialized in genetic diseases.
"I was in charge of outpatient care for pediatric patients with genetic disorders. I saw many patients who, despite seeing numerous doctors, still had undiagnosed conditions. Although I was able to diagnose some patients due to my extensive experience in the US, there were many cases where a diagnosis couldn't be made, so my primary focus was carefully examining the patients' symptoms and listening to their stories and those of their families. The process involved hypothesizing about potential diseases based on symptom combinations and then checking each relevant gene one by one for mutations—it was a time-consuming and meticulous process in those early days."
As the number of patients increased, a new Center for Medical Genetics was established in 2011, dedicated to diagnosing, studying, and providing education on genetic disorders throughout the entire hospital. The center now operates with a team of four doctors and two nurses. Around this time, news emerged from outside Japan about the potential of next-generation sequencing (NGS)—a technology for analyzing the whole genome—as a valuable tool for diagnosing rare genetic diseases in patients for whom traditional clinical examinations had failed to diagnose. This method also revealed that it could lead to the discovery of entirely new diseases, ones so rare that only a handful of cases were known globally.
"The human genome contains roughly 3 billion DNA bases, or ‘letters.’ Next-generation sequencers can read all 3 billion of these letters indiscriminately to analyze the entire human genome. After extracting chromosomes from patient cells and slicing them using ultrasound, the process involves determining the sequence of hundreds of DNA letters within the resulting fragments. This data is then compared to the standard human DNA sequence, fitting the sequence from the patient into the human genome as if assembling a puzzle. Additionally, by comparing the patient's DNA sequence with that of their parents, we can identify which gene or which specific change in the DNA sequence is causing the disease.”
However, conducting this process, known as genomic analysis, requires complex computer programs, presenting a high barrier to entry for many researchers. Fortunately, these programs were written on UNIX, an operating system with which Prof. Kosaki had some experience. The computer skills he had taught himself during his student years as a resident proved invaluable, allowing him to quickly embrace this emerging field of genomic disease research.

Prof. Kosaki's interest in computer programming began in middle school at Keio Futsubu School (Boys Junior High School), sparking a lifelong fascination with technology.
"After entering university, I spent about two years focusing on programming before beginning my formal studies in the medical sciences. Back then, personal computers were still called ‘microcomputers.’ Although I had fewer opportunities to code after I became a resident, I discovered that a nearby engineering university in the northern Kanto area where I was training had a large computer system. After some persuasion, they let me access the system through a phone line.”
The large computer ran on the UNIX, the leading operating system at the time. Today, UNIX is used in most scientific programming, but Prof. Kosaki’s experience of learning basic UNIX commands over a dial-up internet connection would later prove invaluable for genome analysis.
“I never imagined that something I casually picked up as a hobby would become such a powerful research tool 30 years later."
Discovering New Diseases Through Genome Analysis
Through the genetic analysis of numerous undiagnosed patients, Prof. Kosaki's research group became the first in the world to identify mutations in genes such as PDGFRB, CDC42, CNOT2, CDK19, CTR9, CRMP2, and DHX9 as causes of certain diseases. For example, Prof. Kosaki and Toshiki Takenouchi, an assistant professor in Keio's pediatrics department, discovered that multiple patients with similar combinations of symptoms had mutations in the CDC42 gene. This disease was subsequently named "Takenouchi-Kosaki syndrome" and designated as a rare pediatric disease (specific chronic pediatric disease) eligible for government support.
"This disease is characterized by slight differences in the process by which cells extend their 'arms' due to variations in the CDC42 gene. For instance, nerve cells involve forming networks with their surroundings. In platelets, it's the mechanism by which they extend as they are produced and released into the bloodstream. However, because of congenital differences in this process, the formation of neural networks in the brain may vary, and the size of platelets can be affected."
This rare disease, which affects only about five people in Japan and around twenty globally, arises from an overactivity in the function of the CDC42 gene.
"The increased activity of the CDC42 gene was discovered through basic research by a professor at Kobe University. Their findings suggest that suppressing CDC42 might lead to a potential treatment."

IRUD Launched: Causes Found for Approximately Half of Undiagnosed Patients
Following the discovery of the Takeuchi-Kosakisyndrome, Professor Kosaki felt compelled to expand a project nationwide that would reduce the number of undiagnosed patients through genome analysis. With support from many collaborators, the Initiative on Rare and Undiagnosed Diseases (IRUD) was launched in 2015 as a flagship project of the Japan Agency for Medical Research and Development (AMED). This initiative allows hospitals and researchers across Japan to share information, providing diagnoses for previously undiagnosed patients and contributing to the development of new treatment methods.
"Now, nine years later, IRUD has developed into a network connecting approximately 400 hospitals, 40 university hospitals and national medical centers, and five genome centers, including Keio University. With about 500 researchers involved, IRUD continues to work toward diagnosing undiagnosed patients across the country. The results have been remarkable, with about half of the 7,000 previously undiagnosed patients receiving diagnoses, shedding light on cases that had once been shrouded in uncertainty.
For many years, IRUD focused on children and patients with undiagnosed conditions and rare diseases. By extending the age range downward, we started thinking about how this approach could be used to identify the causes of conditions in critically ill newborns. Collaborating with Dr. Takenouchi, we created a new nationwide network to investigate these cases using genomic analysis. With just 1cc of blood, it is now possible to conduct a complete genomic analysis for a newborn. Initially, completing an analysis took about six months, but waiting that long wasn't feasible for newborns. Streamlining various processes allowed for analysis within about two weeks under typical circumstances and as quickly as three days with the entire team mobilized."
Over a five-year period, around 400 newborns and their families participated in the project, with a diagnosis rate of about 50%. Among those diagnosed, roughly half experienced progress toward treatment, with some finding new strategies for managing their conditions.

Prof. Kosaki hopes that genome-based healthcare, or "genomic medicine," will become a new and valuable form of medical practice that can benefit society.
"In the past, there was a sense of resignation among both patients and medical professionals, with the belief that since genetic disorders were incurable, there was no point in finding the cause. Yet recently, over 5 percent of roughly 3,000 diseases—though it still falls short of 10 percent—have seen the development of treatments worldwide. I think it would be a mistake to tell a patient they have an incurable disease without first investigating if they fall into this 5–10% range. We’re entering an era where genomic analysis can potentially uncover the cause and lead to treatment options, so as healthcare providers, we need to change our mindset. Patients shouldn’t lose hope, even if the cause of their condition isn't immediately clear. The IRUD network and the network for critically ill newborns have expanded nationwide, so if you suspect that a condition may be a genetic disorder, I encourage you to participate in these projects."
Prof. Kosaki says that nothing he has learned has been wasted, and he enjoys the connections he makes through his research, constantly expanding dynamic new networks as he confronts as-yet-unknown diseases.
"You don't have to do everything on your own. Take time to build a network of people who can support you—it can make all the difference when facing a challenge."
Kenjiro Kosaki
After graduating from the Keio University School of Medicine in 1989, Prof. Kosaki joined the school’s Department of Pediatrics. In 1993, he became a clinical genetics fellow at the University of California, San Diego, and after serving as a visiting researcher at Baylor College of Medicine in 1997, he returned to Keio University School of Medicine in 1998 as an instructor in the Department of Pediatrics. In 1999, he was appointed as an assistant professor through the Pharmacia and Upjohn Fund for Growth and Development Research. He remained at the Department of Pediatrics, first as an assistant professor in 2001, then as an assistant professor in 2003. Starting in 2007, he served as an associate professor in the Department of Pediatrics taking on his current position as Director of the Center for Medical Genetics in 2011. From 2019 to 2023, he served as the President of the Japan Society of Human Genetics and led Human Genetics Asia 2023 as Congress President.
He has also been the President of the Japanese Teratology Society since 2019.
*All affiliations and titles are those at the time of publishing.


